ADHD and Dopamine
The current, generally accepted belief is that ADHD (attention deficit/hyperactivity disorder) is caused by a dopamine imbalance within the brain. However, there is controversy as to whether ADHD is caused by hypodopaminergic functioning or hyperdopaminergic. There are several reasons for this theory. First of all, amongst other things, dopamine is often related to attention and motivation. Another reason is due to the effectiveness of methylphenidate based medication (a.k.a. meth salts). Methylphenidate acts as an dopamine reuptake inhibitor by blocking dopamine transporters. Thus there is more dopamine in the neurons, but the dopamine fires less often.
CD and ADHD
Conduct disorder (CD) is characteristic of socially disruptive, aggressive and usually destructive behavior. Destructive not only to property and others, but to one's own daily life. ADHD is very similar to CD, except there tend to be far less violent tendencies, if any. However, like CD, ADHD can be inhibit one's academic career, occupation, or even social ability. It is believed that CD and ADHD are in essence the same on a neurobiological level, and the only difference comes in upbringing. Individuals who grow up in a high-risk environment are more likely to develop CD rather than ADHD, and visa-versa for a low risk environment. Indeed, the two are so similar that CD is classified as a type of ADHD.
Objective
The objective of Gatzke-Kopp et al's experiment was to try and determine whether ADHD/CD and thus other externalizing disorders such as antisocial personality disorder and borderline personality disorder. The original objective was to compare neurological differences between people with CD and ADHD when dealing with rewards and reward anticipation, however it rather quickly became apparent that this would not be possible since ADHD and CD were so similar. A reward based approach was used because both ADHD and CD are often characterized by impulsivity, that is, the inability to defer gratification, even if doing so will result in a greater reward. In the end, it was decided to use a control group of individuals with no mental disorders. Only males were used because of the small sample size.
Procedure
A sample of twenty-one males between the ages of twelve and sixteen with ADHD/CD were chosen as the experimental group. This was later reduced to nineteen because two of the participants were unable to stay still enough for long enough. A control group of eleven males of the same ages with no mental disorders was also chosen. Any individuals taking any sort of stimulant medication were asked to dis continue use at least thirty-six hours before the test. Previous experiments have shown that there is no appreciable difference between individuals with ADHD who have never taken stimulants, and one who has stopped taking them for thrity-six hours.
Both groups were asked to play three rounds of a simple game. A green square was flashed for 1.2 seconds on either the left or right side (chosen psuedorandomly). The participant would then have to press the appropriate button. If the answer was correct, and a monetary reward was given, then a tone was played for half a second; if the answer was correct, and no reward was given, then a different tone was played for half a second. If the answer was incorrect, then there was no adverse affect.
The game had three rounds. The first round any and all correct answers resulted in a forty cent reward. In the second round, no money was ever rewarded, and in the final round, money was rewarded only part of the time.
Results
The results from the fMRI showed that during the first round when a monetary reward was given, both the control group and the experimental group showed increased activity in their striatum in both the left and right hemispheres. The striatum is a part of the basal ganglia, and is most often associated with motor functions (e.g. movement planning), however, it also deals with executive functioning, reward anticipation, and the processing of unique or novel stimuli. The area is also comprised mainly of medium spiny neurons, which are heavy with dopamine (figure 1).
However, during the non-monetary portion, the control group's anterior cingulate cortex (ACC) was highly activated, however, in the experimental group, the striatum continued to be highly activated. Amongst other things the ACC is used for motivation, task anticipation and error detection. (figure 2 and figure 3)
Conclusions
Ultimately, the experiment did not resolve the hypodopaminergic versus hyperdopaminergic debate. While is is true that dopamine is far more prevelant in the striatum than the ACC, there is no garantee that the neurotransmitter being used is indeed dopamine, since fMRI's can only detect brain activity and not which neurotransmitter is being used.
However, this experiment can give us a great deal of insight into other symptoms of ADHD/CD. The activation of the striatum may help explain the impulsivity of individuals with ADHD/CD. Because the striatum is involved with reward anticipation, its continued activation could mean that the anticipation in someone with ADHD/CD is much greater than in a normal individual, and thus much harder to resist.
It is also interesting to note the lack of activation of the ACC. The ACC is important for error detection and error correction, and thus reinforcement learning (i.e. learning from ones mistakes). This could explain, at least to some degree, why people with ADHD are often disturbing, since they would not have learned to control themselves despite being scolded; perhaps more obviously, though, it may help explain the aggressive tendencies, usually socially related, of individuals with CD in a similar, but more pronounced, way it explains the ADHD disruptive behavior.
References
Gatzke-Kopp, Lisa et al. Neurological Correlates of Reward Responding in Adolescents With and Without Externalizing Behavior Disorders. Journal of Abnormal Psychology. Vol. 18 N.1(2009)
Wikipedia. "File:Dopamineseratonin.gif". http://en.wikipedia.org/wiki/File:Dopamineseratonin.gif
Wikipedia. "Methylphenidate". http://en.wikipedia.org/wiki/Methylphenidate
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000.
Tuesday, April 28, 2009
Monday, April 27, 2009
Could LSD cure your OCD?
(Could 'shrooms' make you less afraid of death?)

When a person is diagnosed with terminal cancer it can result in a drastic change in their behavior as well their outlook on life. Often times the fear of death will overwhelm a patient and they will suffer from chronic depression and anxiety. In 2001 the National Cancer Policy Board of the Institute of Medicine released a search for “novel” approaches to palliative treatment. Palliative treatment is the search for a type of medical care that alleviates or reduces a patient’s emotional and psychological suffering as a result of their terminal illness. Dr. Charles Griffiths, of John Hopkins University responded to this search. He suggested an exploration of the hallucinogenic drug Psilocybin. His hope was that the experience on this drug would reduce a person’s anxiety about their impending death as well as minimize their desire for pain medication. Although the drug will not lessen the physical pain caused by the illness, Girffiths suspects that the patient’s attitude and outlook will change dramatically as a result of the experience, ensuing in a changed perception of their pain.
PSILOCYBIN AND ITS EFFECT ON THE BRAIN:
Psilocybin is a hallucinogenic drug found in psilocybin mushrooms (commonly called ‘magic mushrooms’ or ‘shrooms’). Hallucinogens are generally divided into two groups of alkaloids, tryptamines: including drugs such as Psilocybin, DMT and LSD and phenthylamines: such as mescaline. Tryptamines are a type of alkaloid, generally found in plants, animals and fungi. Hallucinogens, such as Psilocybin have been present in religious ceremonies for hundreds of years. Generally these drugs are restricted by indigenous cultures for highly ritualized sacramental and healing ceremonies.
Psilocybin has the ability to profoundly change one’s state of consciousness. Effects of consumption may include a distorted perception resulting in somatic, visual, olfactory, gustatory and auditory hallucinations. Consumption may also produce a synthesis of random sensory experiences such as ‘tasting colours’. The effects listed are common in serotonergically mediated hallucinogens. These are those receptors that exert their influence on the same receptors that respond to serotonin. The brain receptor that is affected by Psilocybin is called 5-HT2A which is widely dispersed throughout the central nervous system, specifically in serotonin rich areas such as the prefrontal, parietal and somatosensory cortex. Hallucinogens such as LSD and Psilocybin act as full/partial agonists at this receptor, causing an increase in this receptors activity.


Fig. 2 Shows the activation sequence for motor activity and demonstrates the thalamus and its role with the aspects of the prefrontal cortex.
Griffiths’s desire was to research whether profound activation of the serotonin receptor could result in what is considered a primary mystical experience. He also wanted to study whether this experience could have lasting effects on a patient’s attitude toward their illness and their fate. Griffiths organized a double blind study comparing the effects of orally administrated Psilocybin and Methylphenidate (often referred to as Ritalin, a psycho-stimulant prescribed for ADHD and narcolepsy that has a similar onset and duration as Psilocybin).
http://www.blogsforcompanies.com/TTimages/psilocybin_research_study.jpg
The study was designed so that measures were taken, during the drug session, 7 hours after ingestion, two months after ingestion and finally, 14 months after their first Psilocybin trip. The 2 month and 14 month follow up survey assessed altered states of mind, sensitivity to hallucinogen, the scale of one’s mystical experience, changes in attitude and behaviour, spiritual transcendence and personality factors such as neuroticism and openness. Finally, three adults who had been submitted by the participant answered a questionnaire on the participant’s behavior since the experiment.
(Could 'shrooms' make you less afraid of death?)
When a person is diagnosed with terminal cancer it can result in a drastic change in their behavior as well their outlook on life. Often times the fear of death will overwhelm a patient and they will suffer from chronic depression and anxiety. In 2001 the National Cancer Policy Board of the Institute of Medicine released a search for “novel” approaches to palliative treatment. Palliative treatment is the search for a type of medical care that alleviates or reduces a patient’s emotional and psychological suffering as a result of their terminal illness. Dr. Charles Griffiths, of John Hopkins University responded to this search. He suggested an exploration of the hallucinogenic drug Psilocybin. His hope was that the experience on this drug would reduce a person’s anxiety about their impending death as well as minimize their desire for pain medication. Although the drug will not lessen the physical pain caused by the illness, Girffiths suspects that the patient’s attitude and outlook will change dramatically as a result of the experience, ensuing in a changed perception of their pain.
PSILOCYBIN AND ITS EFFECT ON THE BRAIN:
Psilocybin is a hallucinogenic drug found in psilocybin mushrooms (commonly called ‘magic mushrooms’ or ‘shrooms’). Hallucinogens are generally divided into two groups of alkaloids, tryptamines: including drugs such as Psilocybin, DMT and LSD and phenthylamines: such as mescaline. Tryptamines are a type of alkaloid, generally found in plants, animals and fungi. Hallucinogens, such as Psilocybin have been present in religious ceremonies for hundreds of years. Generally these drugs are restricted by indigenous cultures for highly ritualized sacramental and healing ceremonies.
Psilocybin has the ability to profoundly change one’s state of consciousness. Effects of consumption may include a distorted perception resulting in somatic, visual, olfactory, gustatory and auditory hallucinations. Consumption may also produce a synthesis of random sensory experiences such as ‘tasting colours’. The effects listed are common in serotonergically mediated hallucinogens. These are those receptors that exert their influence on the same receptors that respond to serotonin. The brain receptor that is affected by Psilocybin is called 5-HT2A which is widely dispersed throughout the central nervous system, specifically in serotonin rich areas such as the prefrontal, parietal and somatosensory cortex. Hallucinogens such as LSD and Psilocybin act as full/partial agonists at this receptor, causing an increase in this receptors activity.
Fig.1 The distribution of Serotonin in the brain.
Psilocybin and other hallucinogens are proven to stimulate specific areas of the brain. PET scans show the prefrontal cortex and the amygdala are affected by Psilocybin. The effect on the amygdala explains the heightened emotions one experiences on a Psilocybin 'trip', the prefrontal cortex is responsible for our executive functions and this explains effects on our personality and on our ability to organize thoughts and actions.
There is a great deal of speculation that the thalamus is intensely affected by hallucinogens. The thalamus is a relay station for the previously mentioned 2HT serotonin receptors. It is also responsible for receiving auditory, somatosensory and visual sensory signs. It then sends these sensory signals to the cerebral cortex. If the thalamus were overwhelmed, it may no longer be able to filter through the sensory information properly. This would mean that the prefrontal cortex would be inundated with sensory information. This avalanche of sensory data may be what leads to changes in our behaviour and perception.
Psilocybin and other hallucinogens are proven to stimulate specific areas of the brain. PET scans show the prefrontal cortex and the amygdala are affected by Psilocybin. The effect on the amygdala explains the heightened emotions one experiences on a Psilocybin 'trip', the prefrontal cortex is responsible for our executive functions and this explains effects on our personality and on our ability to organize thoughts and actions.
There is a great deal of speculation that the thalamus is intensely affected by hallucinogens. The thalamus is a relay station for the previously mentioned 2HT serotonin receptors. It is also responsible for receiving auditory, somatosensory and visual sensory signs. It then sends these sensory signals to the cerebral cortex. If the thalamus were overwhelmed, it may no longer be able to filter through the sensory information properly. This would mean that the prefrontal cortex would be inundated with sensory information. This avalanche of sensory data may be what leads to changes in our behaviour and perception.
Fig. 2 Shows the activation sequence for motor activity and demonstrates the thalamus and its role with the aspects of the prefrontal cortex.
THE STUDY:
Griffiths’s desire was to research whether profound activation of the serotonin receptor could result in what is considered a primary mystical experience. He also wanted to study whether this experience could have lasting effects on a patient’s attitude toward their illness and their fate. Griffiths organized a double blind study comparing the effects of orally administrated Psilocybin and Methylphenidate (often referred to as Ritalin, a psycho-stimulant prescribed for ADHD and narcolepsy that has a similar onset and duration as Psilocybin).
The study involved two or three 8 hour drug sessions conducted at 2 month intervals. Thirty-six volunteers aged between twenty-four and sixty-four years were involved. Volunteers were all physically and psychologically healthy, had no previous experience with hallucinogens and were affiliated with some sort of religion/spirituality. Participants were required to have religious/spiritual connections because Griffiths felt it would, “better equip volunteers to understand and consolidate any mystical-type experiences they might have in the study.” Thirty of the thirty-six participants were divided into two groups. On their first drug session the group received a dose of either Methylphenidate or Psilocybin, the alternative drug was administrated to them during their second session. The 8hr drug sessions were conducted in a room designed to replicate a living room.
http://www.blogsforcompanies.com/TTimages/psilocybin_research_study.jpg
Fig.3 The location used for the experiment, a room made to look like a living room.
This comfortable space was to ensure physical safety and a relaxing environment that would not seem threatening in case of hallucinations/perceptual changes. During each drug session the participant was accompanied by two monitors. Sessions were videotaped and participants were encouraged to listen to music, lie down on a couch and wear an eye-mask. In order to decrease the effects of this “expectancy” both the monitor and the subject were “blinded” to what drug was being consumed. Not only that, but a ‘red herring’ group of 6 participants who only received a placebo, but were informed that they had consumed Psilocybin on their third drug session, were a part of the study.
RESULTS:
RESULTS:
The study was designed so that measures were taken, during the drug session, 7 hours after ingestion, two months after ingestion and finally, 14 months after their first Psilocybin trip. The 2 month and 14 month follow up survey assessed altered states of mind, sensitivity to hallucinogen, the scale of one’s mystical experience, changes in attitude and behaviour, spiritual transcendence and personality factors such as neuroticism and openness. Finally, three adults who had been submitted by the participant answered a questionnaire on the participant’s behavior since the experiment.
The most striking result from the survey done 7 hours after drug ingestion, was from the measure of mystical experience questionnaire. This showed that 22 of the 36 volunteers fulfilled the criteria for a ‘complete mystical experience’ as defined by Pahnke and Richards. Findings from the questionnaire 2-months after the drug was ingested express that Psilocybin significantly increased ratings of mood, behaviour, positive attitude and social effect. Sixty seven percent of the participants went on to list their experience on Psilocybin to be one of the most meaningful experiences of their lives or among the top five most meaningful experiences they have ever had.
Fig. 4 Graphs demonstrating results from the 2 month survey and the 14 month survey, comparing the Psilocybin experience and effects with the Methylphenidate experience and effect.
The 14 month follow up survey showed that 64% of the patients indicated the experience as increasing their life satisfaction and well being moderately or very much. Furthermore, 61% described the experience as being associated with significant or extreme, positive changes in behaviour and attitude, since the first session. Since the Psilocybin experience, the volunteers rated low on neuroticism and negative affect and high on extroversion, openness, agreeableness and measure of actualization potential, this rating is based on adult norms. Quotes from the verbatim study that was taken included:
- The experience expanded my conscious awareness permanently...I accept 'what is', more easily.
- That in every horrible or frightening experience, if you stay with it, enter into it, you will find God...It has become a guiding principal in my life.
- I experienced the utter joy of letting go-without anxiety-without direction-beyond ego.
WHAT THIS MEANS:
These results certify that under the correct conditions, Psilocybin is able to be administered safely and that it will successfully produce occurrences similar to spontaneous mystical experiences. The information also confirms that these experiences have a proven long-term positive effect on the lives of participants. Griffith’s hope is to continue his research as this study is only at its preliminary stages. Already, the search for terminal cancer patients, suffering from depression and anxiety and willing to try Psilocybin has begun. He is also hopeful that this drug may aid in treating drug dependency. This is partially inspired by a Canadian study, from the 60’s, that attempted (with some success) to cure alcoholism with Mescaline and LSD.
Griffiths also wishes to investigate the importance of using volunteers with some sort of religious/spiritual connection in order to successfully achieve a ‘mystical experience’ that has long-term effects. Not only does this experiment aid Dr. Griffiths’ own research but it also is helping to re-open the exploration of psychedelic drugs and their potential for the medical world. Studies of these drugs have been off limits for the last few decades, due to their role in the 60’s counter culture, but with the success of experiments like this one, other more radical experiments are being approved, such as a study at UCLA researching LSD and if it could help people with extreme cases of OCD.
Saturday, April 25, 2009
Lie To Me

Background
Relevant Parts of the Brain
Anterior Cingulate Cortex:
- Connected with the prefrontal and parietal cortex
- Regulates autonomic function including blood pressure and heart rate
- Also involved in rational cognitive functions such as reward-anticipation, decision making, empathy and emotion

Dorsal Lateral Prefrontal Cortex:
- Responsible for motor planning, organization and regulation
- Associated with Working-memory; the storage and manipulation of information

The Parietal Cortex:
- Determination of spatial sense and navigation

The Polygraph
- Inadmissible in court
- Federal Polygraph Handbook:
- Question Form - Be clear and concise; Avoid legal terms when possible; Be constructed so that they may be answered yes or no; Not be worded in the form of an accusation or contain an inference that presupposes knowledge or guilt; In specific issue tests when testing for multiple items or amounts of money, use the phrase, "any of', e.g., "Did you steal any of that money?"; In specific issue tests, only address one issue in each question; In specific issue tests, only address one incident in each series.
- Question Type - Primary Relevant. This question tests the possible direct involvement of the examinee. In PDD screening questioning formats, all relevant questions are considered primary relevant questions;
- Secondary Relevant. This question tests the examinee's possible involvement in the
offense under investigation. A secondary relevant question should be constructed to address a secondary issue such as help, plan, or participate; test for secondary involvement in, such as seeing, hearing, or knowing; or focus on the nature or location of evidence and/or physical acts that support the primary offense. There are three types of secondary relevant questions: - 1. Evidence-Connecting. An evidence-connecting question is designed to
determine if the examinee was involved with any of the evidence of the crime or is aware of the nature or location of various items of evidence.
Do you know where any of that money is now? - 2. Guilty-Knowledge. A guilty-knowledge relevant question is used to determine
if the examinee has any knowledge of who committed the incident under investigation.
- 3. Secondary-Involvement. A secondary-involvement relevant question tests for
secondary involvement such as seeing or hearing or focuses on physical acts that support the primary offense.
- Comparison Question. Physiological responses of comparison questions are
compared to physiological responses of relevant questions. The comparison question is designed to produce a greater physiological response for the non-deceptive person. The probable lie and directed lie questions are the two types of comparison questions used within the Federal Government. - 1. Probable-Lie Comparison Question. This question is designed to be a probable lie
for the examinee. The PLC question should be similar in nature but unrelated by time, place or category to the specific issue. However, in screening examinations the PLC can be related to the issue(s) as long as the screening comparison question establishes a dichotomy between the relevant and comparison issues. A comparison question should be broad in scope and time so that it captures as many of the examinee's past life experiences as possible. The physiological responses to the PLC are compared to the responses of the designated relevant questions. The exclusionary and screening comparison questions are the two types of PLC questions used within the federal government.
- 2. Exclusionary Comparison Question (ECQ). A probable-lie question
should be similar in nature but unrelated to the issue being tested. The question should be
separated from the relevant issue by time, place or category. The comparison question should use the same action verb or similar in nature action verb as that of the relevant issue. A comparison question should be broad in scope and time so that it captures as many of the examinee's past life experiences as possible.
- Directed-Lie Comparison. The DLC question is a specialized comparison
question. A properly constructed DLC question involves a minor transgression which should have some personal significance to the examinee. Upon acknowledging having committed such a transgression, the examinee is directed to lie when asked that question on the test. The question is separated from the relevant issue by category.
- Sacrifice Relevant Question. When used, this is the first question that refers to the
relevant issue, and it prepares the examinee for the introduction of the relevant questions.
Sacrifice relevant questions are not scored during the test data analysis phase of a PDD
examination.
- Symptomatic Question. This question is designed to test for an outside issue that
could be more significant for an examinee than the relevant and comparison issues. Symptomatic question responses are evaluated, though not numerically scored, during the test data analysis phase of a PDD examination.
- Stimulus Questions: designed to measure capacity for response. These can be relevant or irrelevant:
Were you on that bridge that night?
- What do the question formats mean?
- The yes/no format means the linguistic construction is always in the hand of the examiner, not the examinee.
- The built in shifts from relevant to irrelevant to comparison and control questions indicate an acknowledgment of the difficulty of maintaining accuracy and control in the testing environment.
- Problems with the Polygraph:
- For instance, using the Directed-Lie Comparison question as an example of how the subject lies poses several real problems since Polygraph measures physiological response and not neurological response. The form of a directed lie question dictates that the subject is instructed to lie. The point of polygraph is to discern a lie based on a spike in stress levels resulting from the concealment of a lie. The Comparison question removes the element of concealment and therefore removes exactly what the examiner wishes to observe: the effects of concealment.
- The problems with Polygraph tests are well known to most people today, they measure stress without having a way of differentiating between the stress caused by crafting a lie and the stress caused by being subjected to a polygraph.
- Langleben: "Its specificity is limited because it relies on the correlates of peripheral nervous system activity, while deception in a cognition event with top-down control by the central nervous system"
- This is the shift his research is trying to make: from physiology to cognition.
The Experiment
Subjects: 23 right-handed male undergraduate students (mean age: 19.36)
Task: A modification of the Guilty Knowledge Task (GKT)
- Instruction Protocol:
- Participants were given an envelope with two playing cards, a 5 of clubs and a 7 of spades, along with $20.
- The investigator instructed the participants to deny possession of one of the cards and acknowledge possession of the other during the imaging phase.
- Participants were told they could keep the money only if they successfully concealed the identity of the lie card during the scan session.
- A third party then led them to the scanner and instructed them to answer each question as truthfully as possible.
- A sequence of photographed playing cards was presented
- The series of cards included five stimulus classes:
- 1. Lie (5 of clubs or 7 of spades)
- 2. Truth (5 of clubs or 7 of spades)
- 3. Recurrent distracter (2 of hearts)
- 4. Variant distracter (remaining cards, 2- 10 all suits)
- 5. Null (back of card)
- Cards were presented for 2 seconds followed by a variable (0 -16 s) during which the null card was shown.
- 24 Lie, Truth and recurrent distracter cards and 168 variant distracter cards were shown.
- Participants were instructed to press a left button (yes) to confirm that a card was in their possession or the right button (no) to deny it.
- In total, 432 stimuli were presented with a session length of 14.4 minutes.
- Results:








- No difference between those who reported using a strategy and those who reported using no strategy.
- "The key point is that you need to exercise a system that is in charge of regulating and controlling your behavior when you lie more than when you just say the truth," Langleben said. "Three areas of the brain generally become more active during deception: the anterior cingulated cortex, the dorsal lateral prefrontal cortex and the parietal cortex."


1. The initial ACC and inferior parietal lobe findings are not replicated and the frontal activations described are of insufficient statistical significance to be reported by most neuroimaging groups (Z values of less than 3);
2.The parietal lobes (bilaterally) now exhibit greater activation during truthful responding than deceptive responding (c.f. Langleben et al., 2002); and
3.The behavioural and functional anatomical findings are reported differently across the 2005 papers: while truthful RTs appear only qualitatively longer than lie responses in Langleben et al. (2005), they are reported as significantly longer in Davazitkos et al. (2005); while very many regions exhibit greater activation during truthful responding in Langleben et al. (2005), a different subset of foci are maximally informative in Davazitkos et al. (2005; admittedly, following application of a different, and novel, analytic method)."
Conclusion
- Admits that brain activity previously associated with deception was driven by the task design
- Lie and Truth operate with a similar frontoparietal network, but lie still appears to be a more working-memory associated task
Langleben, et. al. Telling Truth From Lie in Individual Subjects With Fast Event-Related fMRI. University of Pennsylvania, 2005.
Federal Psycho-physiological Detection Of Deception Examiner Handbook. COUNTERINTELLIGENCE FIELD ACTIVITY TECHNICAL MANUAL October 2,2006
Temple-Raston. Neuroscientist Uses Brain Scan to See Lies Form. http://www.npr.org/templates/story/story.php?storyId=15744871. NPR, 2009.
Spence, Sean. Playing Devil's Advocate: The Case against fMRI Lie Detection. Legal and Criminal Psychology (2008) 13, 11-25. The British Psychological Society, 2008.
Friday, April 24, 2009
Chelsey Article
here is the link ot my article...
http://discovermagazine.com/2008/jun/16-could-an-acid-trip-cure-your-ocd
http://discovermagazine.com/2008/jun/16-could-an-acid-trip-cure-your-ocd
Monday, April 13, 2009
Religious Relaxation
When God Makes a Difference
The study conducted by McGregor, Nash, and Hirsh was based around the idea that religious conviction provided a level of certainty and relief from error, which allows those who are strong believers to ignore the inconsistencies that cause people anxiety. Their hypothesis stated that there was a neurophysiological reason for this decrease in anxious feelings, lying in the reduction of activity in the Anterior Cingulate Cortex.
What’s up the ACC?

The Anterior Cingulate Cortex or ACC is a part of the forebrain located at the frontal part of the cingulated cortex, which lies above the corpus callosum. The ACC is a part of a variety of autonomic functions including blood pressure and heart rate as well as some processes involved in language production and acquisition as we’ve read about in the most recent T. Deacon chapters. However in this study the focus lay on the role of the ACC in more rational cognitive processes such as reward and anticipation and their role in the generation of anxious feelings. Much of the ACCs involvement in error processing lies in its activity in comparing what the intended outcome of a situation is and the actual out come, the ACC responds to an error by aiding in the production of anxious feelings, which allow the subject to become both consciously and physically aware of the error.
The ACC is connected to the prefrontal cortex, parietal cortex, and motor system. It is thus connected to the general system for regulating and modifying behavior. This regulation occurs in reaction to various anxiety producing events such as “the omission of error, the detection of conflict, or the experience of uncertainty.” They believe this to be true because those who are deeply involved in religion have provided for themselves a set of predictive guidelines for the world and occurrences therein. Religions provide meaning systems and moral parameters that the practitioner may operate within they are essentially guides for action and the perception of the actions of others. Anxiety is often caused by a dissonance between the expected action or situation and what actually occurs, those who seriously practice religion however are given rules that “constrain thought and perception away from discrepant or erroneous predictions”, they are able to ignore that which does not fit the teachings of their religion. The conscious reinterpretation of out of the religious box events into preexisting convictions acts as a sort of natural anti-anxiety medication, deadening the ACCs alarm bell for errors.
Study #1
The first study used twenty-eight subjects who came from Christian, Muslim, Hindu, Buddhist, and other religious backgrounds (including non-religious). The researchers had them complete scaled that measured their personality, need for cognitive closure, behavioral inhibition and activation, as well as on their religious zeal. The religious zeal scale, on which they focused, had items that ranged from “I aspire to live and act according to my religious beliefs” to “I would support a war that defended my religious beliefs”. The participants were given a Stroop test, which consisted of a series of color words, each presented in a color that either matched or mismatched the meaning of the word. They were asked to respond to each word by pressing a button that either matched the color of the word or the color the word represented.
To determine the ACC activity they measured event-related potential “which reflects the summation of the postsynaptic potentials of a large ensemble of synchronously active neurons” called the errorealted negativity or ERN. “The ERN is a sharp negative voltage deflection that typically peaks within 50 to 100 ms postresponse and reflects the preconscious monitoring of error, conflict, and uncertainty localized to the ACC “

The results showed that those who were more religiously zealous had less ERN activity, when an error was made the ACC did not react so strongly that they had a feeling of anxiety or any related emotion in making a mistake. They also found that the more zealous a participant was the less errors they made, they were more deliberate and careful in their answers. However the more zealous participants also answered questions faster suggesting a higher level of automatic thoughts, which allow them to answers quickly with more certainty.
Study #2
The second study consisted of twenty-two participants whose religious preferences were not recorded. They were asked to complete a scale on their belief in God as well as an IQ test and the Big Five inventory, which measures five broad categories of personality traits. They also completed a similar Stroop test.

The results of the second study revealed, just as in the first, that a stronger belief in God led to les ERN activity as well as less incorrect answers. Having belief in God is most certainly a less intense form of religious zeal, however this did not diminish the fact that the participants had less anxiety related activity in their ACC.
These results suggest that religious conviction provides a framework for understanding and behavioral activity in the world, thus acting as a buffer against the anxiety provoking situations as well as “minimizing the experience of error”.
Though these studies are based around religious constructs there is a strong possibility that conviction to any ideology could provide similar results.
Carter CS, Braver TS, Barch DM, Botvinick MM, Noll D, Cohen JD. Anterior cingulate cortex, error detection, and the online monitoring of performance. Science 1998; 280: 747–9.
MacDonald, Angus W., et al. "Dissociating the Role of the Dorsolateral Prefrontal and Anterior Cingulate Cortex in Cognitive Control." Science 288.5472 (2000): 1835-8.
The study conducted by McGregor, Nash, and Hirsh was based around the idea that religious conviction provided a level of certainty and relief from error, which allows those who are strong believers to ignore the inconsistencies that cause people anxiety. Their hypothesis stated that there was a neurophysiological reason for this decrease in anxious feelings, lying in the reduction of activity in the Anterior Cingulate Cortex.
What’s up the ACC?

The Anterior Cingulate Cortex or ACC is a part of the forebrain located at the frontal part of the cingulated cortex, which lies above the corpus callosum. The ACC is a part of a variety of autonomic functions including blood pressure and heart rate as well as some processes involved in language production and acquisition as we’ve read about in the most recent T. Deacon chapters. However in this study the focus lay on the role of the ACC in more rational cognitive processes such as reward and anticipation and their role in the generation of anxious feelings. Much of the ACCs involvement in error processing lies in its activity in comparing what the intended outcome of a situation is and the actual out come, the ACC responds to an error by aiding in the production of anxious feelings, which allow the subject to become both consciously and physically aware of the error.
The ACC is connected to the prefrontal cortex, parietal cortex, and motor system. It is thus connected to the general system for regulating and modifying behavior. This regulation occurs in reaction to various anxiety producing events such as “the omission of error, the detection of conflict, or the experience of uncertainty.” They believe this to be true because those who are deeply involved in religion have provided for themselves a set of predictive guidelines for the world and occurrences therein. Religions provide meaning systems and moral parameters that the practitioner may operate within they are essentially guides for action and the perception of the actions of others. Anxiety is often caused by a dissonance between the expected action or situation and what actually occurs, those who seriously practice religion however are given rules that “constrain thought and perception away from discrepant or erroneous predictions”, they are able to ignore that which does not fit the teachings of their religion. The conscious reinterpretation of out of the religious box events into preexisting convictions acts as a sort of natural anti-anxiety medication, deadening the ACCs alarm bell for errors.
Study #1
The first study used twenty-eight subjects who came from Christian, Muslim, Hindu, Buddhist, and other religious backgrounds (including non-religious). The researchers had them complete scaled that measured their personality, need for cognitive closure, behavioral inhibition and activation, as well as on their religious zeal. The religious zeal scale, on which they focused, had items that ranged from “I aspire to live and act according to my religious beliefs” to “I would support a war that defended my religious beliefs”. The participants were given a Stroop test, which consisted of a series of color words, each presented in a color that either matched or mismatched the meaning of the word. They were asked to respond to each word by pressing a button that either matched the color of the word or the color the word represented.
To determine the ACC activity they measured event-related potential “which reflects the summation of the postsynaptic potentials of a large ensemble of synchronously active neurons” called the errorealted negativity or ERN. “The ERN is a sharp negative voltage deflection that typically peaks within 50 to 100 ms postresponse and reflects the preconscious monitoring of error, conflict, and uncertainty localized to the ACC “

The results showed that those who were more religiously zealous had less ERN activity, when an error was made the ACC did not react so strongly that they had a feeling of anxiety or any related emotion in making a mistake. They also found that the more zealous a participant was the less errors they made, they were more deliberate and careful in their answers. However the more zealous participants also answered questions faster suggesting a higher level of automatic thoughts, which allow them to answers quickly with more certainty.
Study #2
The second study consisted of twenty-two participants whose religious preferences were not recorded. They were asked to complete a scale on their belief in God as well as an IQ test and the Big Five inventory, which measures five broad categories of personality traits. They also completed a similar Stroop test.

The results of the second study revealed, just as in the first, that a stronger belief in God led to les ERN activity as well as less incorrect answers. Having belief in God is most certainly a less intense form of religious zeal, however this did not diminish the fact that the participants had less anxiety related activity in their ACC.
These results suggest that religious conviction provides a framework for understanding and behavioral activity in the world, thus acting as a buffer against the anxiety provoking situations as well as “minimizing the experience of error”.
Though these studies are based around religious constructs there is a strong possibility that conviction to any ideology could provide similar results.
Carter CS, Braver TS, Barch DM, Botvinick MM, Noll D, Cohen JD. Anterior cingulate cortex, error detection, and the online monitoring of performance. Science 1998; 280: 747–9.
MacDonald, Angus W., et al. "Dissociating the Role of the Dorsolateral Prefrontal and Anterior Cingulate Cortex in Cognitive Control." Science 288.5472 (2000): 1835-8.
Amygdala Medial Prefrontal Cortex Disconnect
A great amount of research has been conducted exploring how sleep deprivation weakens systems such as the immune system, weight control, cognitive processing (memory and learning) but there has been little inquiry into how sleep loss effects our emotional brain. Sleep deprivation has been commonly associated with several psychiatric disorders. It is thought that psychiatric and mood disorders, such as bi polar disorder, cause sleep loss. However, Mathew Walker and colleagues new study show that this isn’t necessarily the case as sleep deprivation, as the results from their study indicate, can itself be the cause of psychological instability.
The Study:
The study involved 26 healthy participants ages 18-30. The 26 subjects were divided in two groups: 12 were assigned to a sleep control group and the other 14 to a sleep deprivation group. All subjects had to refrain from ingesting caffeinated and alcoholic beverages for a total of 72 hours and followed a normal sleep/wake pattern for one week prior to the study (7 to 9 hours of sleep per night, waking hours: 6am -9pm). Their sleep/wake pattern was monitored by an actigraphy, a wristwatch movement sensor.
Pre-Study:
The sleep control group subjects had a normal night of sleep the night before the scanning. The sleep deprivation group remained awake for the entire night and the entire day before the scanning at 5pm (total of 35 hours of sleep deprivation).
Study/ fMRI Scanning:
The subjects were shown 100 images ranging from neutral to gruesome (i.e. basket on table to images of burn victims). Each image was shown for 10 seconds and the subjects were asked to quickly rate their emotional response through a button system, this was also to insure that all subjects remained awake and alert during the experiment. The subjects were in fMRI scanners during this whole process. Mathews and his colleagues were particularly looking for reactions in the amygdala, and curious to see if there were any significant differences between the sleep control group and the sleep deprivation group.
Results:
Both groups had similar emotional responses to the neutral images, but as the images became more and more aversive the fMRI scans showed that there were indeed great differences in how the brains were firing in the sleep-deprived subjects. In both groups the amygdala, as hypothesized, showed greater activity in response to the intense images, yet the sleep deprived subjects amygdala’s were 60% more active than the sleep control group subjects. Not only were the sleep deprived subjects amygdalas showing a stronger activation but also the volume of the amygdala that was activated (greater amount of neurons being activated) was three times that of the sleep control subjects.

It also became evident when observing the fMRI scans that there was a difference in the brain wiring of the control subjects and the sleep control subjects. The control subjects amygdalas maintained normal communication with the medial-prefrontal cortex (MPFC), however; the sleep deprivation participants amygdalas appeared to have lost connectivity with the MPFC and were instead communicating with regions of the autonomic nervous system.

Why is this loss of connectivity with the MPFC significant?
The MPFC communicates with the amygdala as it sends connections to the amygdalas central nucleus and brain stem outputs of the central nucleus. The MPFC serves as an “inhibitory, top-down control of amygdala function, resulting in contextually appropriate emotional responses.”


Maria Morgan, working in Joseph LeDoux’s lab, researched damaged MPFC and found that some lesions of MPFC resulted in exaggerated fear reactions. When the amygdala is reacting to fear the MPFC remains inactive and vice versa. When the MPFC is damaged increased anxiety occurs as the amygdala is left “unchecked” by the MPFC. This often leads to a difficulty with decision making in emotional situations. This research supports Mathews and colleagues’ findings. However, in their case study a lack of connectivity between the MPFC and amygdala wasn’t caused by lesions in the MPFC but rather by a lack of sleep.

The heightened emotional state occurs when threatening or in this case disturbing stimuli goes unchecked by the MPFC, and this greater activation of the amygdala communicates with the autonomic nervous system that in turn can lead to fight or flight responses.
Stimuli that activate the fight or flight response trigger the brains periventricular system PVS, commonly known as the brains punishment circuit. The PVS is composed of the hypothalamus, the thalamus, and the gray substance around the Sylvius. Acetylcholine activates emission of a hormone known as adrenal cortico-trophic ACTH which activate the adrenal glands to release adrenalin that prepares the body for fight or flight response.
This case study highlights the great importance of sleep. While more research must be done on the connection of sleep deprivation and mood disorders it is clear that sleep loss affects those without symptoms of psychiatric disorders as well. Most of us have experienced the altered state after pulling an all nighter. Now there is evidence that our brains are literally rewiring to create a heightened emotional state. As more research is conducted sleep might be taken more seriously in terms of psychological instabilities. Perhaps certain careers that often keep employees awake for hours on end who’s decision making is crucial will be reconsidered. For example, medical workers.
Sources:
LeDoux, Joseph. Synaptic Self: How Our Brains Become Who We Are. New York: Penguin Books, 2002.
Swaminathan Nikhil. “Can a Lack of Sleep Cause Psychiatric Disorders? Study shows that sleep deprivation leads to a rewiring of the brain’s emotional circuitry” Scientific American. October 23 2007. Get link
Walker, Mathew P. et al. “The human emotional brain without sleep- a prefrontal amygdala disconnect.” Current Biology. Vol 17 No 20.
Walker, Mathews P. et al “ Supplemental Data: The human emotional brain without sleep- a prefrontal-amygdala disconnect” Current Biology. Vol 17 No 20.
“The Amygdala and its Allies.” The Brain from Top to Bottom
http://thebrain.mcgill.ca/flash/i/i_04/i_04_cr/i_04_cr_peu/i_04_cr_peu_1a.jpg
The Study:
The study involved 26 healthy participants ages 18-30. The 26 subjects were divided in two groups: 12 were assigned to a sleep control group and the other 14 to a sleep deprivation group. All subjects had to refrain from ingesting caffeinated and alcoholic beverages for a total of 72 hours and followed a normal sleep/wake pattern for one week prior to the study (7 to 9 hours of sleep per night, waking hours: 6am -9pm). Their sleep/wake pattern was monitored by an actigraphy, a wristwatch movement sensor.
Pre-Study:
The sleep control group subjects had a normal night of sleep the night before the scanning. The sleep deprivation group remained awake for the entire night and the entire day before the scanning at 5pm (total of 35 hours of sleep deprivation).
Study/ fMRI Scanning:
The subjects were shown 100 images ranging from neutral to gruesome (i.e. basket on table to images of burn victims). Each image was shown for 10 seconds and the subjects were asked to quickly rate their emotional response through a button system, this was also to insure that all subjects remained awake and alert during the experiment. The subjects were in fMRI scanners during this whole process. Mathews and his colleagues were particularly looking for reactions in the amygdala, and curious to see if there were any significant differences between the sleep control group and the sleep deprivation group.
Results:
Both groups had similar emotional responses to the neutral images, but as the images became more and more aversive the fMRI scans showed that there were indeed great differences in how the brains were firing in the sleep-deprived subjects. In both groups the amygdala, as hypothesized, showed greater activity in response to the intense images, yet the sleep deprived subjects amygdala’s were 60% more active than the sleep control group subjects. Not only were the sleep deprived subjects amygdalas showing a stronger activation but also the volume of the amygdala that was activated (greater amount of neurons being activated) was three times that of the sleep control subjects.

It also became evident when observing the fMRI scans that there was a difference in the brain wiring of the control subjects and the sleep control subjects. The control subjects amygdalas maintained normal communication with the medial-prefrontal cortex (MPFC), however; the sleep deprivation participants amygdalas appeared to have lost connectivity with the MPFC and were instead communicating with regions of the autonomic nervous system.

Why is this loss of connectivity with the MPFC significant?
The MPFC communicates with the amygdala as it sends connections to the amygdalas central nucleus and brain stem outputs of the central nucleus. The MPFC serves as an “inhibitory, top-down control of amygdala function, resulting in contextually appropriate emotional responses.”
Maria Morgan, working in Joseph LeDoux’s lab, researched damaged MPFC and found that some lesions of MPFC resulted in exaggerated fear reactions. When the amygdala is reacting to fear the MPFC remains inactive and vice versa. When the MPFC is damaged increased anxiety occurs as the amygdala is left “unchecked” by the MPFC. This often leads to a difficulty with decision making in emotional situations. This research supports Mathews and colleagues’ findings. However, in their case study a lack of connectivity between the MPFC and amygdala wasn’t caused by lesions in the MPFC but rather by a lack of sleep.
The heightened emotional state occurs when threatening or in this case disturbing stimuli goes unchecked by the MPFC, and this greater activation of the amygdala communicates with the autonomic nervous system that in turn can lead to fight or flight responses.
Stimuli that activate the fight or flight response trigger the brains periventricular system PVS, commonly known as the brains punishment circuit. The PVS is composed of the hypothalamus, the thalamus, and the gray substance around the Sylvius. Acetylcholine activates emission of a hormone known as adrenal cortico-trophic ACTH which activate the adrenal glands to release adrenalin that prepares the body for fight or flight response.
This case study highlights the great importance of sleep. While more research must be done on the connection of sleep deprivation and mood disorders it is clear that sleep loss affects those without symptoms of psychiatric disorders as well. Most of us have experienced the altered state after pulling an all nighter. Now there is evidence that our brains are literally rewiring to create a heightened emotional state. As more research is conducted sleep might be taken more seriously in terms of psychological instabilities. Perhaps certain careers that often keep employees awake for hours on end who’s decision making is crucial will be reconsidered. For example, medical workers.
Sources:
LeDoux, Joseph. Synaptic Self: How Our Brains Become Who We Are. New York: Penguin Books, 2002.
Swaminathan Nikhil. “Can a Lack of Sleep Cause Psychiatric Disorders? Study shows that sleep deprivation leads to a rewiring of the brain’s emotional circuitry” Scientific American. October 23 2007. Get link
Walker, Mathew P. et al. “The human emotional brain without sleep- a prefrontal amygdala disconnect.” Current Biology. Vol 17 No 20.
Walker, Mathews P. et al “ Supplemental Data: The human emotional brain without sleep- a prefrontal-amygdala disconnect” Current Biology. Vol 17 No 20.
“The Amygdala and its Allies.” The Brain from Top to Bottom
http://thebrain.mcgill.ca/flash/i/i_04/i_04_cr/i_04_cr_peu/i_04_cr_peu_1a.jpg
Friday, April 10, 2009
Thursday, April 9, 2009
Tuesday, March 31, 2009
Autism and Music
Autism Spectrum disorders affect about 6 in every 1,000 people with varying severities. The prevalence has been drastically increasing since the 1980’s, but most people believe that is not due to an actual increase in the disorder but simply a change in diagnostic criteria.
Autism starts affecting children before the age of three. It is characterized by difficulty with social interactions, repetitive behaviors, and difficulty in acquiring and using language. About 0.5% to 10% of autistic individuals are called autistic savants. They are extremely gifted in one skill set or talent. Though scientists are not in agreement with the causes of autism, there are many theories that dominate the general discourse. It is commonly assumed to be a combination of environmental and genetics with differing emphasis between the two. The research that is compelling for the genetics autism paradigm involves studies of identical twins which proved that there was a 60% chance that the twin of an autistic child would develop autism. These results are staggering considering that .6% of the population has autism and fraternal twins showed no significant increase in autism prevalence.
Further, many researchers have found physical irregularities in several parts of the brain including the levels of serotonin in the brain. Specifically, research centers called “Centers of Excellence in Autism Research” have shown that connections in the brain are often impaired in autistic children. “Research is now being conducted all over the world to determine specific genes that increase the likelihood of someone developing autism. A group known as the International Molecular Genetic Study of Autism Consortium, which includes clinicians and researchers from the USA, UK, France, the Netherlands, Denmark, Italy, and Greece, has pinpointed four chromosomes which they believe play critical roles in autism. The chromosomes they identified are numbers 2, 7, 16 and 17. The evidence for involvement of chromosomes 2 and 7 is particularly strong as these had also been previously identified by other independent researchers (2,3,4,5). Chromosome 7 is known to be associated with many language disorders and chromosome 2 plays an important role in early brain development. These findings are further demonstrated by research showing dyslexia patients also have abnormalities on these chromosomes. This is not surprising as dyslexia also produces deficits in learning ability and information processing in the brain”
The problem with autism is something that we take for granted. Most of us learn how to make sense of our environment through an unconscious ability to combine our sensory information. What we hear, see, feel and know all merge to create spatial maps that allow us to understand our relative place in space. In childhood, we learn how to put our senses together to respond more efficiently to impediments presented to us in our environment. Children with autism have trouble learning to do this. They have greater difficulty creating a synthesis of all the sensory information and therefore have more difficulty responding to the environmental impediments. Sensory integration therapy is a type of occupational therapy that places children in a room specifically designed to stimulate and challenge all of the senses. This therapy is based on the assumption that the child is either overstimualted or understimulated by the environment. Specifically music therapy seeks to stimulate the auditory processing in autistic children so that the overall sensory integration will be more efficient. Music therapy seeks to regulate a common trend in autism; acute lack of total sensory integration. This is reflected and materialized in many ways in the brain.
Auditory Processing of Music
The majority of symptoms in children and adults include attention deficits, learning disabilities, autism, obsessive-compulsive disorder, depression, anxiety, chronic pain and many more are all directly a result of an imbalance of electrical activity in the brain. There are many environmental factors that can produce an imbalance of electrical activity and function of the two sides of the brain documented as either an increase of activity on one side or a decreased activity on the other.
Adverse activity is the right hemisphere which autism is expected to be specifically stimulated by low frequency tones, negative or d ownbeat music. Specifically, autism is a common sensory processing disorder (SPD). In children with autism, sensory integration is very difficult to accomplish. Music therapy can work as a way to increase the integration of the main sensory areas. The sensory system is broken up into three main areas: the tactile, vestibular, and the proprioceptive sense. The tactile system is your sense of touch. The vestibular system is responsible for movement and the body’s position in space. The proprioceptive system deals with muscles and joints. There are other sensory systems but they are not as commonly associated with sensory dysfunction.
ownbeat music. Specifically, autism is a common sensory processing disorder (SPD). In children with autism, sensory integration is very difficult to accomplish. Music therapy can work as a way to increase the integration of the main sensory areas. The sensory system is broken up into three main areas: the tactile, vestibular, and the proprioceptive sense. The tactile system is your sense of touch. The vestibular system is responsible for movement and the body’s position in space. The proprioceptive system deals with muscles and joints. There are other sensory systems but they are not as commonly associated with sensory dysfunction.
The vestibulocochlear system informs us of sound, movement and orientation of space. The cochlear portion of the system turns sound or vibration into electrochemical messages that are relayed throughout the central nervous system and is critical to auditory processing. The vestibular portion serves to provide stabilization, influences attention and arousal, posture, movement, thus being critical to sensorimotor integration. It is the integration of our senses that allows us to understand what we are experiencing in our world.
Specifically, the vestibular system contributes to our balance and our sense of spatial orientation that provides input about movement and equi librioception. (equilibrioception is what experiencial information from the vestibular system is called.) It is anatomically joined with cochlear system, and the systems lie closely together throughout the nervous system and together elaborate the general labyrinth of the inner ear.
librioception. (equilibrioception is what experiencial information from the vestibular system is called.) It is anatomically joined with cochlear system, and the systems lie closely together throughout the nervous system and together elaborate the general labyrinth of the inner ear.
Further, there is a profound connection between vestibular functioning and language processing. This allows for many close neuronal associations with auditory processing and language. The vestibular system sends signals primarily to the neural structures that control our eye movements, and to the muscles that keep us upright.
Decreased vestibular processing can impact on the area of speech and language development, particularly auditory processing. It is associated with autistic disorder, which are generally categorized by decreased electrical neurotransmitting activity. Research has found that therapy to improve the function of the vestibular system can also result in improved language development.
Musical Processing and Emotional Understanding
Vestibular complications are not the only ways that music can affect autism. A benefit to music therapy for autistic children aids them in verbal communication and social interaction deficits. A proposed study by Molnar Szakacs and Overy wants to compare musical processing on a neurological basis to communication, language and action. This is determined by the mirror neuron system, which allows us to abstract musical sounds similar to the ways in which humans form language when speaking and interacting. “The mirror neuron system has been proposed as a mechanism allowing an individual to understand the meaning and intention of a communicative signal by evoking a representation of that signal in the perceivers own brain “(p.235.) Spatial maps created in the brain, specifically the parietal lobe, are influenced by these mirror neurons and contribute to an overall understanding of actions and intentions. Essentially, mirror neurons enable humans to understand emotions through facial and body expressions.
Music is closely connected with motor activity. Producing music involves developed spatial maps and a physical understanding of vibrations and sounds. The mirror neuron system that allows someone to understand musical experiences is the same set of neurons that is present in motor functioning and mapping. There have been recent neuro-imaging studies that show that people with musical expertise have a change in their fronto-parietal mirror neuron system. Music is also inherently similar to language. Music is pitches composed into symphonies the way that language is words composed into novels.
The proposed study by Molnar Szakacs emphasizes the important connection between an understanding of language with an understanding of music. This is further emphasized by research conducted on other language disorders like dyslexia. The main point that Molnar Szakacs intends to look at is if language and music are so similar and if they are dictated by similar mirror neural patterns, then why can’t autistic savants with high pitch sensitivity understand facial emotions and social communications?
Mirror neurons are cells that enable normally developing people to decipher meaning and intention in actions as well as replicate those actions. Autistic children are typically noted to have a decreased or altered mirror neural system. This affects the ways in which the limbic system, which is responsible for emotions, interacts with those mirror neurons. This comes back to the point that these same mirror neurons are involved in the understanding of music.
Music Based Therapies
Autism starts affecting children before the age of three. It is characterized by difficulty with social interactions, repetitive behaviors, and difficulty in acquiring and using language. About 0.5% to 10% of autistic individuals are called autistic savants. They are extremely gifted in one skill set or talent. Though scientists are not in agreement with the causes of autism, there are many theories that dominate the general discourse. It is commonly assumed to be a combination of environmental and genetics with differing emphasis between the two. The research that is compelling for the genetics autism paradigm involves studies of identical twins which proved that there was a 60% chance that the twin of an autistic child would develop autism. These results are staggering considering that .6% of the population has autism and fraternal twins showed no significant increase in autism prevalence.
Further, many researchers have found physical irregularities in several parts of the brain including the levels of serotonin in the brain. Specifically, research centers called “Centers of Excellence in Autism Research” have shown that connections in the brain are often impaired in autistic children. “Research is now being conducted all over the world to determine specific genes that increase the likelihood of someone developing autism. A group known as the International Molecular Genetic Study of Autism Consortium, which includes clinicians and researchers from the USA, UK, France, the Netherlands, Denmark, Italy, and Greece, has pinpointed four chromosomes which they believe play critical roles in autism. The chromosomes they identified are numbers 2, 7, 16 and 17. The evidence for involvement of chromosomes 2 and 7 is particularly strong as these had also been previously identified by other independent researchers (2,3,4,5). Chromosome 7 is known to be associated with many language disorders and chromosome 2 plays an important role in early brain development. These findings are further demonstrated by research showing dyslexia patients also have abnormalities on these chromosomes. This is not surprising as dyslexia also produces deficits in learning ability and information processing in the brain”
The problem with autism is something that we take for granted. Most of us learn how to make sense of our environment through an unconscious ability to combine our sensory information. What we hear, see, feel and know all merge to create spatial maps that allow us to understand our relative place in space. In childhood, we learn how to put our senses together to respond more efficiently to impediments presented to us in our environment. Children with autism have trouble learning to do this. They have greater difficulty creating a synthesis of all the sensory information and therefore have more difficulty responding to the environmental impediments. Sensory integration therapy is a type of occupational therapy that places children in a room specifically designed to stimulate and challenge all of the senses. This therapy is based on the assumption that the child is either overstimualted or understimulated by the environment. Specifically music therapy seeks to stimulate the auditory processing in autistic children so that the overall sensory integration will be more efficient. Music therapy seeks to regulate a common trend in autism; acute lack of total sensory integration. This is reflected and materialized in many ways in the brain.
Auditory Processing of Music
The majority of symptoms in children and adults include attention deficits, learning disabilities, autism, obsessive-compulsive disorder, depression, anxiety, chronic pain and many more are all directly a result of an imbalance of electrical activity in the brain. There are many environmental factors that can produce an imbalance of electrical activity and function of the two sides of the brain documented as either an increase of activity on one side or a decreased activity on the other.
Adverse activity is the right hemisphere which autism is expected to be specifically stimulated by low frequency tones, negative or d
ownbeat music. Specifically, autism is a common sensory processing disorder (SPD). In children with autism, sensory integration is very difficult to accomplish. Music therapy can work as a way to increase the integration of the main sensory areas. The sensory system is broken up into three main areas: the tactile, vestibular, and the proprioceptive sense. The tactile system is your sense of touch. The vestibular system is responsible for movement and the body’s position in space. The proprioceptive system deals with muscles and joints. There are other sensory systems but they are not as commonly associated with sensory dysfunction.The vestibulocochlear system informs us of sound, movement and orientation of space. The cochlear portion of the system turns sound or vibration into electrochemical messages that are relayed throughout the central nervous system and is critical to auditory processing. The vestibular portion serves to provide stabilization, influences attention and arousal, posture, movement, thus being critical to sensorimotor integration. It is the integration of our senses that allows us to understand what we are experiencing in our world.
Specifically, the vestibular system contributes to our balance and our sense of spatial orientation that provides input about movement and equi
librioception. (equilibrioception is what experiencial information from the vestibular system is called.) It is anatomically joined with cochlear system, and the systems lie closely together throughout the nervous system and together elaborate the general labyrinth of the inner ear.Further, there is a profound connection between vestibular functioning and language processing. This allows for many close neuronal associations with auditory processing and language. The vestibular system sends signals primarily to the neural structures that control our eye movements, and to the muscles that keep us upright.
Decreased vestibular processing can impact on the area of speech and language development, particularly auditory processing. It is associated with autistic disorder, which are generally categorized by decreased electrical neurotransmitting activity. Research has found that therapy to improve the function of the vestibular system can also result in improved language development.
Musical Processing and Emotional Understanding
Vestibular complications are not the only ways that music can affect autism. A benefit to music therapy for autistic children aids them in verbal communication and social interaction deficits. A proposed study by Molnar Szakacs and Overy wants to compare musical processing on a neurological basis to communication, language and action. This is determined by the mirror neuron system, which allows us to abstract musical sounds similar to the ways in which humans form language when speaking and interacting. “The mirror neuron system has been proposed as a mechanism allowing an individual to understand the meaning and intention of a communicative signal by evoking a representation of that signal in the perceivers own brain “(p.235.) Spatial maps created in the brain, specifically the parietal lobe, are influenced by these mirror neurons and contribute to an overall understanding of actions and intentions. Essentially, mirror neurons enable humans to understand emotions through facial and body expressions.
Music is closely connected with motor activity. Producing music involves developed spatial maps and a physical understanding of vibrations and sounds. The mirror neuron system that allows someone to understand musical experiences is the same set of neurons that is present in motor functioning and mapping. There have been recent neuro-imaging studies that show that people with musical expertise have a change in their fronto-parietal mirror neuron system. Music is also inherently similar to language. Music is pitches composed into symphonies the way that language is words composed into novels.
The proposed study by Molnar Szakacs emphasizes the important connection between an understanding of language with an understanding of music. This is further emphasized by research conducted on other language disorders like dyslexia. The main point that Molnar Szakacs intends to look at is if language and music are so similar and if they are dictated by similar mirror neural patterns, then why can’t autistic savants with high pitch sensitivity understand facial emotions and social communications?
Mirror neurons are cells that enable normally developing people to decipher meaning and intention in actions as well as replicate those actions. Autistic children are typically noted to have a decreased or altered mirror neural system. This affects the ways in which the limbic system, which is responsible for emotions, interacts with those mirror neurons. This comes back to the point that these same mirror neurons are involved in the understanding of music.
Music Based Therapies
So it makes sense that a program that would stimulate and help to integrate the cochlear and vestibular systems might be very helpful for the autistic child’s emotional understanding. This does not present a cure for autism, but The Listening Program (TLP) can be an effective intervention for children on the autistic spectrum.
TLP is a music-based sound stimulation program that currently consists of 8 one hour audio CD’s that contain specially processed classical music and nature sounds plus a 112 page guidebook. Listening sessions are typically fifteen minutes in length, done once or twice a day, five days a week, using high quality stereo headphones.
1- Increases engagement- The individuals experience an improvement in their self-image and an improved sense of their body in space. This enables them to feel more comfortable interacting with their surroundings. They show an increase in the toleration and need for physical contact. There is also an increase in attentiveness and initiation of eye contact.
2- Emerging Skills- When used in conjunction with other forms of therapy, it allows for better integration of the motor and sensory systems which in turn leads to a faster rate of skill acquisition.
3- Auditory Processing- It improves the accuracy and speed at which individuals process sound. This leads to better overall communication skills.
4- Reduced Sound Sensitivity- Many autistic individuals experience hypersensitivity to sounds because their nervous system is unable to regulate the sensory input. This program helps the nervous system be able to better process sensor info, which reduces sound sensitivity.
TLP is a music-based sound stimulation program that currently consists of 8 one hour audio CD’s that contain specially processed classical music and nature sounds plus a 112 page guidebook. Listening sessions are typically fifteen minutes in length, done once or twice a day, five days a week, using high quality stereo headphones.
1- Increases engagement- The individuals experience an improvement in their self-image and an improved sense of their body in space. This enables them to feel more comfortable interacting with their surroundings. They show an increase in the toleration and need for physical contact. There is also an increase in attentiveness and initiation of eye contact.
2- Emerging Skills- When used in conjunction with other forms of therapy, it allows for better integration of the motor and sensory systems which in turn leads to a faster rate of skill acquisition.
3- Auditory Processing- It improves the accuracy and speed at which individuals process sound. This leads to better overall communication skills.
4- Reduced Sound Sensitivity- Many autistic individuals experience hypersensitivity to sounds because their nervous system is unable to regulate the sensory input. This program helps the nervous system be able to better process sensor info, which reduces sound sensitivity.
Monday, March 30, 2009
Obesity: Reviving the Promise of Leptin
The History of Leptin
- Discovered by Douglas Coleman (The Jackson Laboratory, Bar Harbor, Maine)
- Parabiosis of normal mice with either diabetic or overweight mice.
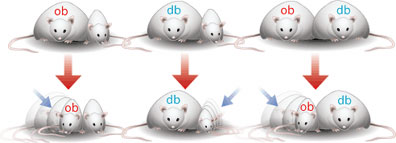
- Found that there was a "satiety factor" circulating in the blood. Hypothesized that db mice lacked the receptor to the factor, while ob mice did not produce it.
- It could not be extracted from the blood because it was present in tiny amounts. However, the gene responsible for it was eventually isolated and the "satiety factor", leptin, was produced in a lab. The leptin gene is spliced into bacteria and the bacteria sets to work producing the protein.
- By the mid 1990s it was greeted as a possible miracle cure for the rising obesity epidemic. 1995 New York Times headline read: "Researchers find hormone causes a loss of weight". Leptin is discussed as a "magic bullet", which would hopefully "change the image of obesity, helping people to see it not as a punishment for gluttony but rather as a metabolic disorder, treatable with a remedial hormone just as diabetes is treated with insulin."
- By the end of 90s none of the new research had panned out. All experiments that had been done on obese humans had found that leptin rarely caused weight loss, and if it did it was only temporary. New York Times headline from 1999 read: "Hormone that slimmed fat mice disappoints as panacea in people". Researchers determined that obese people were somehow resistant to leptin, so it was not effective in their brain.
- Since then most research has focused on understanding the metabolic pathways of leptin, and little thought has been given as to how it might be used as a treatment for obesity.
- Hypothalamus is the main organ involved in regulation of appetite; specifically the arcuate nucleus (situated at the base).
- The neurons involved primarily employ serotonin as a neurotransmitter, although neuropeptide Y and Agouti-Related peptide are also involved.
- The hypothalamus uses Ghrelin, Leptin, Insulin and PYY as markers to influence how hungry we feel.
- Ghrelin is excreted by the stomach may also be produced in the brain. Causes feelings of hunger and is associated with regular meal times. Ghrelin levels rise immediately before a meal and fall sharply after eating.
- Ghrelin Factoids: Those suffering from anorexia nervosa have higher blood levels of ghrelin. - Individuals who have undergone gastric bypass surgery produce less ghrelin. - Ghrelin acts not only on neurons in the arcuate nucleus but also activates reward circuitry in the brain associated with dopamine.

- Leptin is mainly produced by white adipose tissue. Leptin blood level is proportional to body fat. The more body fat on the body the more leptin that is produced.
- When leptin is given to genetically obese mice they lose 30% of their body weight in 2 weeks. When leptin is given to lean mice they lost all their body fat in 4 days.
- Human trials with leptin were unsuccessful. Except at the highest doses (several tablespoons a day) there were no significant changes in weight.
- Why was it so unsuccesful? Obese humans develop a resistancy to leptin in their brain.
- Umut Ozcan - Harvard - Endoplasmic Reticulum Stress Plays a Central Role in Development of Leptin Resistance
- General Hypothesis: The hypothalamus has become resistant to leptin through a process called Endoplasmic Reticulum Stress (ER Stress) which ultimately results in reduced ER function. This causes reduced function of Leptin Receptor signaling. To resensitize the brain to leptin it is necessary to improve function in the ER. Chemical chaperones have been shown to do this.

- The Endoplasmic Reticulum is an organelle responsible for protein folding and transportation of proteins to the cell membrane.
- If the normal processes of the ER are disturbed misfolded proteins accumulate in the cell. This activates cellular stress mechanism called the Unfolded Protein Response (UPR) is activated.
- UPR halts protein translation and causes an increase in the production of molecular chaperones involved in protein folding. If this mechanism is unsuccessful, UPR leads to apoptosis.
- How ER stress is induced and how this leads to UPR is not well understood. The main theory suggests that increased levels of circulating cytokines, fatty acids, excess nutrition and activation of the rapamycin pathway (involved in cellular homeostasis) contribute.
- What they demonstrated in the paper:
- Leptin Acts on a Subset of Hypothalamic neurons
- ER Stress Inhibits Leptin Receptor Signaling
- ER Stress Creates Leptin Resistance in the Brain of Lean Mice
- Improvement of ER Function Enhances Leptin Signaling
- ER Capacity of the Brain Links Obesity to Leptin Resistance
- Chemical Chaperones are Leptin Sensitizers.
2. ER Stress Inhibits Leptin Receptor Signaling
- Cells that presented the Leptin Receptor (LepRB) were exposed to tunicamycin (a chemical that induces ER stress) and then treated with leptin for 45 minutes.
- There was no evidence of leptin-stimulated tyrosine phosphorylation of LepRB or Stat3 phosphorylation (both cellular events that occur as a result of leptin binding to LepRB).


 This indicates that UPR inhibits LepRB signaling at all steps.
This indicates that UPR inhibits LepRB signaling at all steps.
- Since LepRB is folded in the ER they next investigated ER stress blocks LepRB translocation from the ER to the cell membrane as a possible explanation of the block in leptin signaling.
- They induced ER stress in cells using tunicamycin and then used immunflorescence staining to analyze LepRB levels in the cell membrane. They found that ER stress does not decrease LepRB translocation to the membrane nor does it cause a misfolding of LepRB.

3. ER Stress Creates Leptin Resistance in the Brain of Lean Mice
- First - Showed that injecting tunicamycin into the hypothalamus of lean mice caused ER Stress.
- Second - Showed that ER stress in the brain's of lean mice completely blocked activation of Stat3.

- Third - Noted that the food uptake of lean mice with induced ER stress in the hypothalamuc increased.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Bred XNKO mice that produced less of the regulators involved in protein folding in the ER therefore making them more susceptible to ER stress (deletion of the XPB1 gene).
- On a normal diet they had a slightly lower body weight. Blood glucose and leptin levels were normal. Glucose homeostasis was maintained within a normal range.
- On a high fat diet the XNKO mice gained weight more quickly. A sharp increase in leptin level was maintained through out the experiment. They consumed more food, had a higher total fat amount and a significantly lower lean mass.


- These results support the hypothesis that ER capacity of the brain is involved in regulating body weight, leptin sensitivity and metabolic homeostasis.
- Chemical chaperones are compounds that have been found to increase ER function and decrease the accumulation of misfolded proteins in the ER, thereby reducing the likelihood that ER stress will occur.
- 2 FDA approved chemical chaperones for humans are 4-phenyl butyrate (PBA) and tauroursodeoxycholic acid (TUDCA). Past studies have shown that these chemicals can relieve ER stress in the liver and adipose tissues, as well as enhancing insulin sensitivity in mouse models.
- Attempted to reverse ER stress in the hypothalamus of mice who had been on a high fat diet. Normal mice were kept on a high-fat diet for 25 weeks and then treated with PBA for 10 days, followed by daily leptin administration.
- Control mice rapidly lost weight and then rapidly regained it. Mice treated with PBA rapidly loss weight, they also consumed less food.


- Similar results were obtained with TUDCA.
- Both PBA and TUDCA also had some success in increasing leptin sensitivity in genetically obese mice (ob/ob mice).
- After years of searching for leptin-sensitizing agents, chemical chaperones have been identified as potential novel treatment options for obesity.
Sunday, March 29, 2009
Musical Behavior in a Neurogenetic Developmental Disorder
Evidence from Williams Syndrome
Daniel J. Levitin
Daniel J. Levitin's paper reviews a series of studies performed to assess the musical abilities and behaviors of individuals with Williams Syndrome- a neurogenetic developmental disorder.
What is Williams Syndrome (WS)?
Williams Syndrome is created by a small genetic accident which occurs during meiosis, when a segment of DNA containing 25 genes is lost. The result of which affects abstract thought, so that many WS have a bad concept of spacial, quantitative, reasoning, attention, eye-hand coorination, and reading abilities. WS people tend to be very talkative, and will talk with everyone; they completely lack a sense of social fear. Functional brain scans have shown that the amygdala in WS people shows no reaction when they see angry or worried faces.
Here is an image taken from the National Institutes of Health website depicting the difference in amydala activity scanned in reaction to threatening scenes and faces in WS participants and controls (http://www.nih.gov/news/pr/jul2005/nimh-10.htm)
 Abnormal regulation of the amygdala in participants with Williams Syndrome (right) compared to controls (left). The amygdala activates more for threatening scenes (bottom), but less for threatening faces (top).
Abnormal regulation of the amygdala in participants with Williams Syndrome (right) compared to controls (left). The amygdala activates more for threatening scenes (bottom), but less for threatening faces (top).
What is the connection between WS and music?
Not only do WS people show extreme friendliness and near-normal speaking skills, they also tend to be more engaged in musical activities and musicality than others. Levitin reports in this paper a possible neuroanatomical correlate of this engagement, with increased activation in the right amydala to music and to noise.
Based on Levitin and his team's observations, claims of musicality involve many aspects of music including frequent music listening, music performance (for example: a WS person can be able to play the clarinet despite not knowing how to tie their shows) , a deep emotional engagement with msuic, or an above-average musical memory and sound sensitivities (hyperacusis) involving unusual sensitivity to sound, categorization or labelling of sounds that others can't, or anxiety and fear of sounds that non-WS people do not find aversive.
Levitin says that WS can help us better understand the links between genes, brain, and musical behaviors and that WS hypersociability and lack of social inhibitions might be related to their musicality.
The Studies
1st Step:
Characterizing the musical phenotype in WS
The Questionnaire.
Levitin administered a questionnaire to the caregivers of 130 WS participants, 130 Down syndrome participants, 130 autistic participants, and to 130 normal controls. The questionnaire gathered information about physical variables, interest in music, emotional responses to music, musical training, the amount of time engaged in musical activities, and the age of onset of musical activities.
Individuals with WS showed a significantly younger age of onset of musical interest, spent more time per week listenign and playing, and were reported to experience higher levels of emotion when listening to music.
A prinical components analysis revealed seven underlying orthogonal factors that contributed to the profile obtained from the questionnaire. This can be divided up into 7 factors including content related to musical complexity, reproduction, sensitivity, musical theory and achievement, listening habits, positivity, and emotions.
Study of Neural Correlates of Auditory Perception in WS using fMRI
Levitin hypothesized that he would find differences in brain activation bewteen people with WS and controls, and that WS people would show a wider and more diffuse pattern of activation to music and noise stimuli than controls, and that they would show a greater amygdaloidal activation, indexing their heightened emotional reations to music and noise.
Study was conducted usuing a desensitization program that involved a professionally proudced video introdcution to the fMRI scanning procedure, usuing a child's-eye-view of the facility and a child's narration. This was followed to a visit fo an fMRI simulator in which the participants could become acclimated to the noises and enclosed space. 5 WS participants were recruited for an fMRI study of differential processing of music and noise, and five age- and sex-matched controls.
Participants listened to to excerpts from familiar and unfamiliar classical music, as well as the types of noisy sounds that WS people are often sensitive to, such as fans, motors, and leaf blowers.
Results:
Comparing music to noise, WS individuals showed a significantly lower voxel intensity bilaterally in the superior temporal cortex, middle temporal gyri, and superior temporal sulcus. In a comparison of responses to music-minus-rest vs. noise-minus-rest, control participants showed significantly higher temporal lobe activations to the music than the noise, while the WS participants showed virtually indistinguishable activation levels.
He also observed marked differences between WS patients and controls in the right amydala, with WS patients exhibiting far greater activation intensity in the music-minus-noise contrast. This points to a possible neural basis for the unusal acoustical and musical sensitivities observed in affected individuals. Overall, WS participants showed more variable and diffuse activations throughout the brain, and the showed increased activation in the amygdala and cerebellum.
The test of musical skills:
Rhythmic Production Ability
To test rhthym, Levitin and his team presented 8 WS individuals and 8 mentally age-matched controls with a set of clapped rhythums in increasing complexity. The participant had to clap back the rhythm as accurately as possible. Independent coders, blind to hypothesis, and group membership, analyized audio tapes of the test sessions and scored each trial as correct or incorrect or incorrect but very musical nonetheless.
The results showed that the WS and control participants obtained an equal number of correct trials about 66%. However, WS indiviuduals were three times more likely when incorrect to supply a musically compatible rhythm. This was interpreted as a marker of rhythmic ability or creative rhythmicity among the WS participants.
Melodic Production Ability
Levitin presented 12 WS individuals, 12 chronologically age-matched NCs, and 12 individuals with DS a set of melodies increasing in complexity, to assess their melodic reproduction ability. WS and NC were statistically better at melodic repetition than the DS, and not significantly different from one another. He then presented all participants with a set of melodic fragments and instructed them to complete the melodies. The WS individuals were not as good at melodic completion as the NCs. Thus, WS individuals are better at rhymic production than melodic production.
Sources:
Daniel J. Levitin
Daniel J. Levitin's paper reviews a series of studies performed to assess the musical abilities and behaviors of individuals with Williams Syndrome- a neurogenetic developmental disorder.
What is Williams Syndrome (WS)?
Williams Syndrome is created by a small genetic accident which occurs during meiosis, when a segment of DNA containing 25 genes is lost. The result of which affects abstract thought, so that many WS have a bad concept of spacial, quantitative, reasoning, attention, eye-hand coorination, and reading abilities. WS people tend to be very talkative, and will talk with everyone; they completely lack a sense of social fear. Functional brain scans have shown that the amygdala in WS people shows no reaction when they see angry or worried faces.
Here is an image taken from the National Institutes of Health website depicting the difference in amydala activity scanned in reaction to threatening scenes and faces in WS participants and controls (http://www.nih.gov/news/pr/jul2005/nimh-10.htm)
Abnormal regulation of the amygdala in participants with Williams Syndrome (right) compared to controls (left). The amygdala activates more for threatening scenes (bottom), but less for threatening faces (top).What is the connection between WS and music?
Not only do WS people show extreme friendliness and near-normal speaking skills, they also tend to be more engaged in musical activities and musicality than others. Levitin reports in this paper a possible neuroanatomical correlate of this engagement, with increased activation in the right amydala to music and to noise.
Based on Levitin and his team's observations, claims of musicality involve many aspects of music including frequent music listening, music performance (for example: a WS person can be able to play the clarinet despite not knowing how to tie their shows) , a deep emotional engagement with msuic, or an above-average musical memory and sound sensitivities (hyperacusis) involving unusual sensitivity to sound, categorization or labelling of sounds that others can't, or anxiety and fear of sounds that non-WS people do not find aversive.
Levitin says that WS can help us better understand the links between genes, brain, and musical behaviors and that WS hypersociability and lack of social inhibitions might be related to their musicality.
The Studies
1st Step:
Characterizing the musical phenotype in WS
The Questionnaire.
Levitin administered a questionnaire to the caregivers of 130 WS participants, 130 Down syndrome participants, 130 autistic participants, and to 130 normal controls. The questionnaire gathered information about physical variables, interest in music, emotional responses to music, musical training, the amount of time engaged in musical activities, and the age of onset of musical activities.
Individuals with WS showed a significantly younger age of onset of musical interest, spent more time per week listenign and playing, and were reported to experience higher levels of emotion when listening to music.
A prinical components analysis revealed seven underlying orthogonal factors that contributed to the profile obtained from the questionnaire. This can be divided up into 7 factors including content related to musical complexity, reproduction, sensitivity, musical theory and achievement, listening habits, positivity, and emotions.
Study of Neural Correlates of Auditory Perception in WS using fMRI
Levitin hypothesized that he would find differences in brain activation bewteen people with WS and controls, and that WS people would show a wider and more diffuse pattern of activation to music and noise stimuli than controls, and that they would show a greater amygdaloidal activation, indexing their heightened emotional reations to music and noise.
Study was conducted usuing a desensitization program that involved a professionally proudced video introdcution to the fMRI scanning procedure, usuing a child's-eye-view of the facility and a child's narration. This was followed to a visit fo an fMRI simulator in which the participants could become acclimated to the noises and enclosed space. 5 WS participants were recruited for an fMRI study of differential processing of music and noise, and five age- and sex-matched controls.
Participants listened to to excerpts from familiar and unfamiliar classical music, as well as the types of noisy sounds that WS people are often sensitive to, such as fans, motors, and leaf blowers.
Results:
Comparing music to noise, WS individuals showed a significantly lower voxel intensity bilaterally in the superior temporal cortex, middle temporal gyri, and superior temporal sulcus. In a comparison of responses to music-minus-rest vs. noise-minus-rest, control participants showed significantly higher temporal lobe activations to the music than the noise, while the WS participants showed virtually indistinguishable activation levels.
He also observed marked differences between WS patients and controls in the right amydala, with WS patients exhibiting far greater activation intensity in the music-minus-noise contrast. This points to a possible neural basis for the unusal acoustical and musical sensitivities observed in affected individuals. Overall, WS participants showed more variable and diffuse activations throughout the brain, and the showed increased activation in the amygdala and cerebellum.
The test of musical skills:
Rhythmic Production Ability
To test rhthym, Levitin and his team presented 8 WS individuals and 8 mentally age-matched controls with a set of clapped rhythums in increasing complexity. The participant had to clap back the rhythm as accurately as possible. Independent coders, blind to hypothesis, and group membership, analyized audio tapes of the test sessions and scored each trial as correct or incorrect or incorrect but very musical nonetheless.
The results showed that the WS and control participants obtained an equal number of correct trials about 66%. However, WS indiviuduals were three times more likely when incorrect to supply a musically compatible rhythm. This was interpreted as a marker of rhythmic ability or creative rhythmicity among the WS participants.
Melodic Production Ability
Levitin presented 12 WS individuals, 12 chronologically age-matched NCs, and 12 individuals with DS a set of melodies increasing in complexity, to assess their melodic reproduction ability. WS and NC were statistically better at melodic repetition than the DS, and not significantly different from one another. He then presented all participants with a set of melodic fragments and instructed them to complete the melodies. The WS individuals were not as good at melodic completion as the NCs. Thus, WS individuals are better at rhymic production than melodic production.
Sources:
Levitin, Daniel J. (2005) Musical Behavior in a Neurogenetic Developmental Disorder, Retrieved March 15, 2009 from Daniel J. Levitin's Website: http://www.psych.mcgill.ca/levitin/
Dobbs, David "The Gregarious Brain." The New York Times July 8, 2007. Retrieved on March 15, 2009 from nytimes.com
Subscribe to:
Posts (Atom)